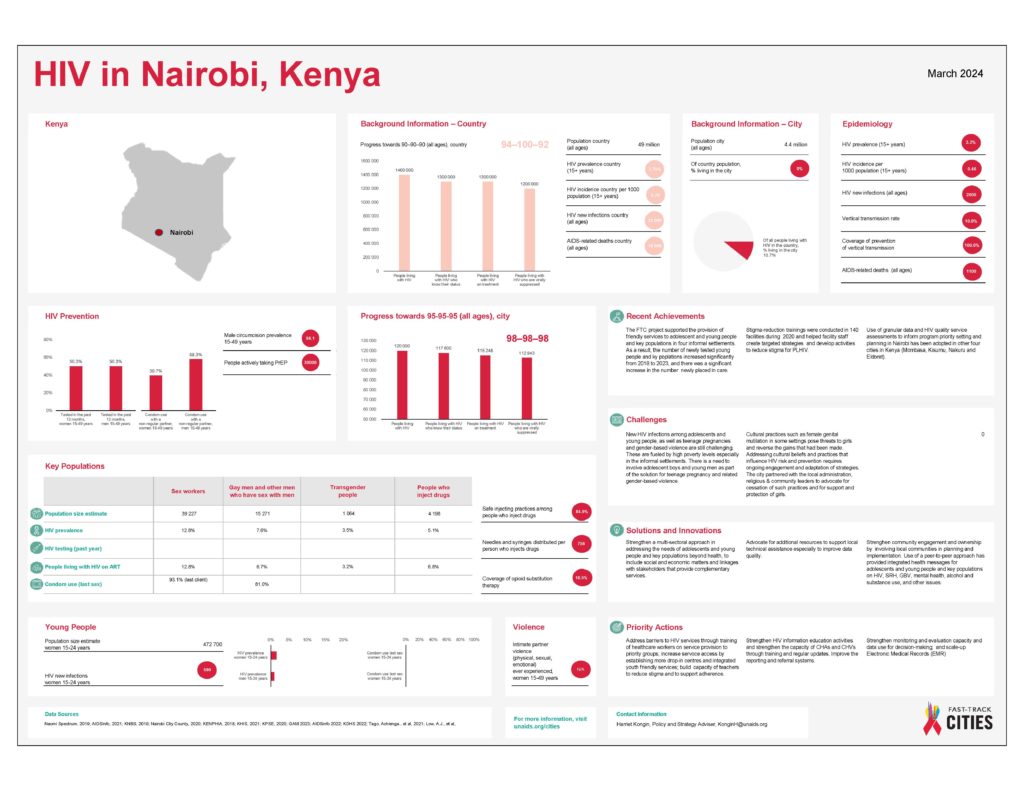
Nairobi is the capital city of Kenya and home to a number of highly mobile populations, including internal migrants and refugees. There are an estimated 191 000 people living with HIV in the city, which accounts for 13% of the national HIV burden. Overall, the city has an adult prevalence of 6%1.
Rapid urbanization and high levels of poverty in informal settlements have contributed to increased risk of HIV transmission in the city. HIV prevalence in informal settlements is almost double that of the city average, while key populations—such as female sex workers and gay men and other men who have sex with men—are particularly vulnerable, with HIV prevalence of 23% and 18%, respectively1. The majority of new HIV infections are estimated to occur among adolescents and young people (46%) and key populations (33%)1.
Nairobi was one of the original signatories of the Paris Declaration in 2014. A city AIDS and TB strategy was developed in 2015, and the city has shown strong commitment to Fast-Track its HIV response. Five years later, Nairobi has made good progress in offering HIV prevention and treatment services, including to key and vulnerable populations: estimated HIV prevalence fell from a high of 14% in the 1990s to 8% in 2013, and then to 6% in 20182. The city HIV testing and treatment targets stand at 78–99–82, while PrEP has been rolled out in close to 80 facilities1,3.
The key to Nairobi City County’s success is its commitment to collecting and using accurate strategic information to understand the HIV epidemic and drive the response.

© Nina R
1 Kenya National AIDS Control Council. Nairobi County: AIDS response progress report, 2018.
2 Spectrum estimates, 2019.
3 Kenya AIDS Indicator Survey (KAIS) 2012 data.
Collecting granular data
In 2017, Nairobi City County authorities collected facility-level data to improve understanding of the HIV epidemic and its response at the local level. All health facilities offering HIV and TB services in the county were mapped, and data were analysed to identify barriers and bottlenecks to service delivery. The exercise showed that 60–70% of Nairobi residents live in about 200 informal settlements that occupy just 6% of the land. These informal settlements were concentrated in four subcounties where HIV prevalence was almost double that of the whole city (12% compared to 6%). HIV prevalence was highest in the informal settlement of Kibera (around 16%)1.
A related mapping exercise was conducted to develop a detailed understanding of the availability and quality of services available for adolescents and young people and key populations in these four subcounties.
Assessing health services
A qualitative assessment of services for adolescents and young people and key populations was done in 24 health facilities: nine that were government-owned, eight that were private and seven run by faith-based organizations. Focus group discussions and interviews were conducted with service users and health workers2.
This assessment made it possible to identify gaps and barriers in service delivery for both groups (adolescents and young people and key populations). While satisfaction was expressed by service users, there were concerns and problems. The assessment showed that less than half of the facilities provided adolescent-friendly services, and that only three facilities offered key population-friendly services. In addition, none of the services met the national standards for comprehensive adolescent-friendly services. Key population-friendly services were only available in private, non-profit organizations and there was an unequal distribution of appropriate services for both groups between the subcounties2.
Overall, adolescents and young people and key populations identified a lack of staff training as a hindrance to providing appropriate services. These groups felt that staff in most health facilities lacked the technical skills, empathy and professionalism required to deal with their particular needs2.
Recommendations to improve the quality of services for these groups included establishing friendly centres in each subcounty, creating functional referral networks, and including peer educators and outreach workers to strengthen services2. The report also recommended specific training for health-care workers who deal with adolescents and young people and key populations, as well as continuous mentorship. All staff on the site—not just health workers—should be sensitized to the special needs of these groups2.
From recommendations to action
The results of the qualitative assessment exercise informed a review of the national guidance on adolescent care, which was conducted with the active participation of adolescents and young people. Fifty health-care workers—including clinical officers, nurses, medical social workers and counsellors—were then sensitized and trained according to the new guidance.
Training on key population services was also conducted for 55 health workers from government health facilities in the four subcounties, with participation from representatives of the communities of sex workers, gay men and other men, who have sex with men, and people who use drugs. Both the training and the participation of the members of key populations challenged the attitudes and prejudices of health workers to great effect, resulting in health-care workers expressing regret about their previous poor attitudes towards (and treatment of) key populations.
Good practices and lessons learned from the adolescent and key population interventions have been documented, and the results will inform the national curriculum on the provision of services for adolescents and young people and key populations.
The Nairobi experience shows the value of strategic information in effecting change. “The evidence was very influential and has mobilized political commitment,” says Carol Ngunu, Deputy Director of Health Service for Nairobi City County. “It has led to a lot of change across the city”3.
1 Granulated facility-based HIV and TB services in Nairobi City County. UNAIDS Kenya; 2018.
2 Qualitative assessment of HIV service delivery in informal settlements in four sub-counties of Nairobi. UNAIDS Kenya, City of Nairobi; 2018.
3 Personal correspondence with Dr Carol Ngunu, October 2018.
Nairobi’s successful HIV response is rooted in strengthened strategic information systems that guide effective policies and planning appropriate to the needs of its populations. Even during the changing contexts triggered by COVID-19, the city has been able to show leadership and continued to respond to these needs.
The achievements and lessons learned through the Fast-Track Cities project in Nairobi have inspired four additional urban centres in Kenya to join the initiative and accelerate their own city HIV responses.
Harnessing data for change
Strategic information, including efficient data collection, has been key to the city’s success, contributing to effective planning and programming in the HIV response. With Fast-Track City support, Nairobi Metropolitan Services (NMS) has invested heavily in human resources, both by increasing the number of health care workers in HIV clinics and data officers, and by providing them with training. It has also invested in tools, including registers and electronic medical records. The data collected at sub-county level are reviewed and shared monthly, with NMS undertaking additional periodic reviews.
In sub-counties and informal settings with high HIV burdens, granular data and qualitative assessments of services for adolescents and young people and key populations have been key in setting priorities and planning improvements for these more vulnerable groups. Health care workers, including community health volunteers, have received additional capacity-building support. The number of health facilities offering integrated and friendly services for young people and members of key populations has increased from zero in 2018 to 22 in 2021. As a result, many more people are being reached with services. Among adolescents and young people, 103,401 were newly tested for HIV in 2021 (compared to 59,643 in 2018) while 11,538 availed themselves of family planning services (compared to 4,139 in 2018). The number of members of key populations newly tested for HIV increased over tenfold in the same period: from 417 to 5,432.[1]
Youth for change
Young people are themselves involved in initiatives for their health and well-being through the youth advisory council that advises NMS on health needs for young people at the community level. Their meaningful engagement in determining priorities and interventions has played a critical role in NMS programmes, including Fast-Track Cities.
In Kawangware – a large, diverse and poor informal settlement, with limited access to basic services including health care – Kawangware Youth for Change is working to create social and behavioural change. The group, founded two years ago and supported by NMS, boasts a football team and holds regular discussions to give young people the opportunity to explore the issues affecting their community. This includes gender issues, such as the role of men in helping their partners to access sexual and reproductive health services.
Members of Kawangware Youth for Change have been trained as “champions” and are leading mobilization and advocacy efforts in their communities. They reach out to peers and other community members to promote use of HIV testing, sexual and reproductive health, and related mental health services among adolescents and young people, as well as members of key populations. They also distribute condoms, placing them in strategic locations.
Adapting to COVID-19
COVID-19 restrictions and shifts in the priorities and focus of city health workers and staff to COVID-19 related activities threatened to disrupt HIV service delivery. Nairobi rapidly introduced a number of contingency plans to divert this threat, including three-month dispensation of HIV medication. Beneficiaries of existing programmes, including trained youth champions and community health workers, were recruited to ensure the continued provision of HIV services, particularly among communities in informal settlements. Meetings and training continued on a virtual basis.
Community ART groups
“Since we formed our ART group, I have never seen anyone defaulting on treatment.” ─ Community health volunteer, Mathare[2]

Government-imposed restrictions to contain the spread of the COVID-19 pandemic included limitations on hospital visits, restricting the ability of people living with HIV to access their medications and continue treatment. In response, Nairobi Metropolitan Services established community ART groups (CAGs) in its sub-counties. These not only maintained access to treatment during the lockdown, but have continued to help men and women living with HIV to receive ART medication within their own communities – cutting the time and financial costs of visiting facilities.
The CAGs are carefully constituted of people living with HIV who are older than 20, have been on treatment for at least a year, who adhere to their medication and do not require frequent follow-up. There is a maximum of 15 members per group and all members should live in the same area, with some places therefore having a number of groups. One of the aims of the CAGs is to provide role models for others in the community to initiate and adhere to treatment. Members are recruited at health facilities where they receive treatment: those who are eligible are informed of the groups and, if they wish to join, are given training from Nairobi City County and the facility. Members are taught about understanding adherence support, follow-up, and basic support in HIV care and treatment.
Every six months a community health volunteer attends a group meeting to distribute medication to all the members. The CAGs also give members the opportunity to share their experiences and lessons of successfully living with the virus, and integrate economic empowerment initiatives such as table-banking to enable members to start small businesses. Through group representatives, health facilities receive reports of the meetings – including on the health and adherence status of members, as well as on any challenges faced – and provide feedback and advice to the group. All members also need to report periodically to their health facility for clinical consultations, on the advice of their health care worker. As a result, very few group members are lost to follow-up or miss recommended tests.
Also key to the success of the CAGs is the engagement of people living with HIV – through platforms established in health facilities to provide opportunities to give feedback on HIV interventions – alongside strong leadership from the NMS. Being part of accountability systems for their health empowers people living with HIV and improves their care.
[1] Nairobi Metropolitan Services. Going beyond the usual: Fast Track Cities 90-90-90 – HIV Stories of Change. 2021.
[2] Nairobi Metropolitan Services. Going beyond the usual: Fast Track Cities 90-90-90 – HIV Stories of Change. 2021.