
The majority (92%) of new HIV diagnoses in the United States occur in 25% of counties, with the southern states disproportionately affected. Three cities—Baton Rouge, Miami and New Orleans—have the highest rates of new HIV diagnoses in the country. The greater New Orleans area, with a population of nearly 800 000 people, has an estimated 7000 people living with HIV1,2. The mayor of New Orleans is committed to accelerating the HIV response and signed the Paris Declaration in April 2016.
HIV transmission in the city occurs mainly among gay men and other men who have sex with men, and men of colour are at particularly high risk. Nearly 80% of new HIV diagnoses between 2013 and 2017 were among men; of those, nearly 70% were among gay men and other men who have sex with men. While HIV treatment and prevention services are available across the city, the testing and treatment targets are 87–66–97, which suggests that there is still some way to go to reach the agreed targets3.
Health experts in New Orleans have recognized that the city’s HIV epidemic needs to be urgently addressed. Key to this is the provision of antiretroviral treatment and the attainment of viral suppression, both for the health benefit of the patient and to prevent further transmission of HIV. Same-day or rapid-start antiretroviral treatment has been effective in getting people living with HIV in care and achieving viral suppression, and there was a need to demonstrate that this approach could be successful in community-based clinics.

1 Local Data: New Orleans (Orleans & Jefferson Parishes). In: AIDSVu [Internet]. AIDSVu; c2019 (https://aidsvu.org/state/louisiana/new-orleans/, accessed 27 August 2019).
2 Halperin J, Butler I, Conner K, Myers L, Holm P, Bartram L et al. Linkage and antiretroviral therapy within 72 hours at a federally qualified health center in New Orleans. AIDS Patient Care STDS. 2018;32(2):2018.
3 New Orleans. In: Fast-Track Cities Global Web Portal [Internet]. IAPAC; c2019 (http://www.fast-trackcities.org/resources/new-orleans, accessed 27 August 2019).
The majority (92%) of new HIV diagnoses in the United States occur in 25% of counties, with the southern states disproportionately affected. Three cities—Baton Rouge, Miami and New Orleans—have the highest rates of new HIV diagnoses in the country. The greater New Orleans area, with a population of nearly 800 000 people, has an estimated 7000 people living with HIV1,2. The mayor of New Orleans is committed to accelerating the HIV response and signed the Paris Declaration in April 2016.
HIV transmission in the city occurs mainly among gay men and other men who have sex with men, and men of colour are at particularly high risk. Nearly 80% of new HIV diagnoses between 2013 and 2017 were among men; of those, nearly 70% were among gay men and other men who have sex with men. While HIV treatment and prevention services are available across the city, the testing and treatment targets are 87–66–97, which suggests that there is still some way to go to reach the agreed targets3.
Health experts in New Orleans have recognized that the city’s HIV epidemic needs to be urgently addressed. Key to this is the provision of antiretroviral treatment and the attainment of viral suppression, both for the health benefit of the patient and to prevent further transmission of HIV. Same-day or rapid-start antiretroviral treatment has been effective in getting people living with HIV in care and achieving viral suppression, and there was a need to demonstrate that this approach could be successful in community-based clinics.
CrescentCare Start Initiative
CrescentCare began as an AIDS service organization in 1985, specializing in care for people living with HIV in New Orleans. It provides free HIV and STI testing, linkage to care and other services (such as PrEP and mental health services). CrescentCare became a federally qualified health centre (FQHC) in 2016, and it is now part of the state-funded national network of community-based facilities.
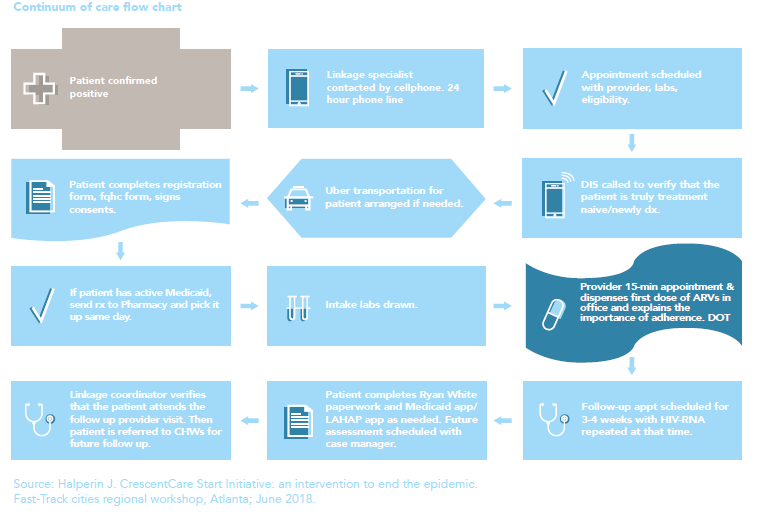
In December 2016, CrescentCare launched a rapid start program. It included two cohorts: the CrescentCare Start Initiative and Early Intervention Services. The CrescentCare Start Initiative linked patients to care and provided antiretroviral therapy within 72 hours, preferably on the same day of diagnosis. Early Intervention Services followed the same protocol for people who were initiating treatment for the first time after 72 hours (with a median of 6 months). They were contacted by the clinic for a first appointment.
In both instances, a coordinator was available 24 hours per day to coordinate the linkage of new diagnoses to care, while the intake process was streamlined to include a focused HIV visit with a treatment provider. An initial visit lasted about 30 minutes, the first dose of antiretroviral therapy was directly observed, and medication for the first 30 days was supplied.
Improved outcomes
To understand the effectiveness of this approach, outcomes were analysed and the continua of care for both cohorts were compared.
A total of 207 patients were followed between December 2016 and April 2018: 136 in the CrescentCare Start Initiative and 71 in the Early Intervention Services. In both cases, about half of the patients were gay men and other men who have sex with men. Around 63% of the CrescentCare Start Initiative group were linked to care within 24 hours of their diagnosis. Viral suppression for those still enrolled in treatment at least one year from linkage was significantly higher in the CrescentCare Start Initiative group (93%) than the Early Intervention Services group (83%). Those in the Early Intervention Services group who were linked to care later also had a lower CD4 count and a higher rate of diagnosed mental illness.
Retention in care was significantly better in the CrescentCare Start Initiative intervention group. It was suggested that this could be explained by: (a) differences in motivation between the two groups; (b) the strong relationship that develops between provider and patient on the day the patient is diagnosed with HIV, starts on antiretroviral therapy and receives counselling on improved health outcomes; or (c) the understanding that U = U4.
The experience of the CrescentCare Start Initiative suggests that a rapid-start antiretroviral therapy model works well in qualified health centres that have extended hours and same-day appointments, and that it presents an opportunity to improve treatment outcomes in similar community settings. Success, however, depends on the availability of a full-time linkage coordinator and the incorporation of a 30-day treatment pack. Provider commitment to this model of care, including flexible scheduling and options for funding access to antiretroviral therapy, is also essential.
1 Local Data: New Orleans (Orleans & Jefferson Parishes). In: AIDSVu [Internet]. AIDSVu; c2019 (https://aidsvu.org/state/louisiana/new-orleans/, accessed 27 August 2019).
2 Halperin J, Butler I, Conner K, Myers L, Holm P, Bartram L et al. Linkage and antiretroviral therapy within 72 hours at a federally qualified health center in New Orleans. AIDS Patient Care STDS. 2018;32(2):2018.
3 New Orleans. In: Fast-Track Cities Global Web Portal [Internet]. IAPAC; c2019 (http://www.fast-trackcities.org/resources/new-orleans, accessed 27 August 2019).
4 Halperin J, Conner K, Butler I, Zeng P, Myers L, Clark R et al. A care continuum of immediate ART for newly diagnosed patients and patients presenting later to care at a federally qualified health center in New Orleans. Open Forum Infect Dis. 2019;6(4):ofz161.